Brain rot: Beware the silent epidemic and reclaim your mind
Brain rot: Beware the silent epidemic and reclaim your mind
Do you ever find yourself mindlessly scrolling on your phone, only to feel empty, unproductive, or more anxious afterward?
You might be experiencing what’s now widely called “brain rot.”
Brain rot is a slang term that went viral on social media and was even named Oxford Word of the Year 2024. It describes the way prolonged exposure to low-quality, fast-paced online content can slow brain function, drain mental energy, and worsen mental health.
Key takeaways
Excessive social media rewires the brain. Constant dopamine hits from endless scrolling can create addiction-like patterns, displacing more meaningful activities
Cognitive and emotional decline. Brain rot shortens attention span, weakens memory, and contributes to anxiety, low mood, and mental fatigue.
Mindful digital habits can reverse the effects. Intentional content choices, screen-time limits, and offline activities help restore focus, emotional balance, and motivation.
Posted on 25 Aug 2025
Written by Dr David Teo, Connections MindHealth
The Science Behind Brain Rot
Dopamine, the brain’s “feel-good” chemical, is released whenever we experience something pleasurable.
Social media platforms are designed to deliver frequent dopamine hits through endless, high-stimulation content. At first, this feels rewarding. Over time, the brain begins to crave constant novelty, rewiring itself in ways similar to behavioural addictions like gambling.
This shift displaces more enriching activities such as reading, exercising, meaningful face-to-face conversations. It leaves us passively consuming random, low-value content that clutters our minds.
Chronic excessive screen time has also been linked to thinning of the cerebral cortex — the area of the brain involved in memory and decision-making.
The Effects of Brain Rot
Excessive short-form video use overstimulates dopamine circuits and alters reward-system activity behaviors resembling gambling or alcohol addiction.
1. Shorter Attention Span
Constant exposure to fast-moving content and frequent digital distractions conditions the brain to expect rapid stimulation. This makes it harder to focus on tasks that require sustained attention, like reading longer texts, finishing detailed work, or staying engaged in conversations. Over time, the brain becomes used to switching quickly between different things. This makes it challenging to maintain deep focus for extended periods.
2. Memory Problems
Frequent interruptions prevent the brain from fully processing and storing information, weakening recall and critical thinking. Without enough focused time, deeper understanding declines.
3. Poor Mental Health
Comparisons to curated online lives and exposure to constant news can fuel anxiety, low mood, and feelings of inadequacy. Using devices late into the night can also disrupt sleep patterns, which in turn increases tiredness, irritability, and worsens emotional regulation.
4. Reduced Cognitive Function & Mental Fatigue
Mindless short-form content can leave you mentally drained, unmotivated, and trapped in a cycle of avoiding challenging mental tasks, further weakening your cognitive abilities.
How Brain Rot Disrupts a Healthy Brain
High screen time in children and young adults is linked to weaker memory, decision-making, and problem-solving.
A healthy brain thrives in three interconnected areas:
Thinking – focus, learning, planning, decision-making, and memory
Feeling – emotional regulation and stress management
Doing – the meaningful activities you engage in each day
Brain rot affects all three, leaving you cognitively dull, emotionally flat, and less motivated to pursue your goals.
The good news: Many of the effects of brain rot can be reversed once healthier habits are restored.
Four Tips to Prevent Brain Rot
Choose Content Wisely: Follow accounts that inspire or educate; mute or unfollow sources of negativity or distraction.
Set Screen-Time Limits: Use built-in controls to stop endless scrolling, especially late at night or when feeling low.
Do More Offline Activities: Rediscover hobbies such as sports, music, art or meeting up with friends for a meal – anything that does not involve a screen.
Scroll With Intention: Before going online, ask: Why am I here? What do I want to find? Don’t get lost in the algorithm.
“Brain rot” may be slang, but it signals a very real challenge in our hyperconnected world. By cultivating mindful digital habits and balancing them with offline life, you can stop the rot and reclaim your mind.
Where to get help:
Mental Well-being
Institute of Mental Health’s Mental Health Helpline: 6389-2222 (24 hours)
Samaritans of Singapore: 1-767 (24 hours) / 9151-1767 (CareText via WhatsApp)
Singapore Association for Mental Health: 1800-283-7019
Silver Ribbon Singapore: 6386-1928
Tinkle Friend: 1800-274-4788
Community Health Assessment Team 6493-6500/1
Counselling
TOUCHline (Counselling): 1800-377-2252
TOUCH Care Line (For Seniors & Caregivers): 6804-6555
Youth suicide is a growing concern in Singapore, with increasing numbers of young people overwhelmed by pressures they struggle to cope with. Hopelessness plays a critical role, as many youths feel trapped in situations they perceive as unchangeable. To prevent these tragedies, it is crucial for families, schools, and communities to foster open communication, ensuring that young people feel supported and understood in their struggles.
Key takeaways
Hopelessness is a key predictor of youth suicide—young people often feel overwhelmed by life stressors and lack coping mechanisms, leading them to believe there is no escape.
The accumulation of pressures—such as academic stress, romantic rejection, family issues, and identity struggles—can push vulnerable youths toward suicidal thoughts.
Open communication and support from families, schools, and communities are critical to preventing youth suicide, helping young people feel seen, heard, and understood.
Posted on 4 Oct 2024
Written by Dr Jared Ng, Connections MindHealth
The heartbreaking rise in youth suicides in Singapore is impossible to ignore. In 2023, nearly 30% of suicides involved individuals under the age of 29, with an alarming number – almost one-third – being children and youths between the ages of 10 and 19. Suicide has tragically become the leading cause of death among our youth, surpassing accidents and illnesses. This devastating reality forces us to confront the intense pressures that many of our young people face every day.
Though the media often refrains from reporting youth suicides, perhaps out of concern for contagion effects or protecting vulnerable individuals, those of us working in mental health witness this silent epidemic. These cases are not just confined to adolescents; even children in primary school are not immune. Behind every statistic is a young life lost, and with it, a family and community left grieving, searching for answers.
The youths who take their own lives often appear to be thriving—excelling academically, socially, and physically. Yet beneath this veneer of success can lie a deep, unnoticed despair that ultimately becomes too much to bear.
The interplay between hope and hopelessness is crucial in understanding youth suicides.
How Hope and Hopelessness Influence Youth Suicide
Hopelessness is a significant factor in suicide risk across all ages, representing a profound state of despair where individuals feel trapped in an unchangeable situation, with suffering that seems endless. This overwhelming sense of hopelessness can lead to the belief that death is the only escape, making it one of the strongest predictors of suicidal behavior. When hope is lost, the risk of suicide dramatically increases.
For young people, hopelessness often stems from life stressors they perceive as insurmountable. Unlike adults, children and youths typically have less experience dealing with complex emotional challenges and may lack the coping mechanisms needed to navigate their despair. Additionally, their natural impulsivity can exacerbate the situation. Young people are more prone to making rash decisions in moments of intense emotion, often without fully considering the consequences. This impulsivity, combined with feelings of hopelessness, can dangerously heighten the risk of suicide, as a young person may act on suicidal thoughts suddenly, leaving little opportunity for intervention.
The interplay between hope and hopelessness is crucial in understanding youth suicides. Hope is a vital psychological resource that begins to develop early in childhood. It starts to form in infancy when a child learns to trust their caregivers and becomes more established around ages 3 to 5, when children develop a sense of purpose and the ability to envision a positive future. However, as children grow older and face more complex social and academic pressures, their sense of hope can be threatened, especially if they encounter repeated failures or rejection. When these pressures become too great, and the child or youth sees no way out, hope can be replaced by hopelessness.
As a parent, it’s essential to understand that even the most successful children can struggle with feelings of inadequacy. Despite outward appearances of success, some youths battle intense internal pressures, setting impossibly high standards for themselves. When they fail to meet these expectations, the resulting feelings of hopelessness, compounded by impulsivity, can lead to a dangerous downward spiral.
Understanding the fragility of hope in our young people is then crucial to grasping the triggers behind youth suicides. But what are these pressures that push them beyond the brink?
Academic pressure is another recurring theme when young people talk about their stressful situations.
Understanding the Triggers Behind Youth Suicide
Through my practice, I’ve encountered many young individuals overwhelmed by circumstances they don’t know how to navigate—circumstances that drive them to contemplate, or even attempt, suicide. One case that stands out is that of a 12-year-old girl whose parents discovered a suicide note hidden in her pencil case. She had poured out her feelings of profound loneliness, all stemming from the rejection of a crush whom she saw as her ‘true love.’ When she tried to talk to her parents about her heartache, they dismissed her emotions, telling her to focus on her studies instead since she was not doing well. For her, this response deepened her isolation. In her note, she expressed that she felt like a burden to her family and believed they would be happier without her. (For the record, this child is alive, and with the support of her parents, she is now receiving the care she needs and is on the path to healing.)
This case, like many others, reminds us that youth suicide is rarely the result of one factor. It’s often an accumulation of pressures—romantic rejection, academic stress, family dynamics, and more. And while romantic relationships are an important part of adolescence, young people’s sense of self-worth is often tied to many areas—be it friendships, peer acceptance, or family approval.
As a mental health professional, cases like this weigh heavily on me. They reinforce how critical it is to listen to our children, even when their struggles seem small to us. This experience, and countless others, have deeply influenced my approach to treating at-risk youths. I’ve learned that what we might dismiss as “typical teenage angst” or fleeting concerns can be the very thing pushing a young person to the edge. Every cry for help, no matter how subtle, deserves to be heard.
I often ask myself, “What can we do better?” or “What more can be done?” In my years of practice, the answer has always come down to fostering connections—helping young people feel seen and heard before their pain becomes too overwhelming to manage. These stories shape the way I approach my work and emphasise the importance of never underestimating the emotional lives of our youths.
Youth suicides are rarely caused by one isolated factor. It’s usually the accumulation of stressors—romantic rejection, academic pressure, and more—that can push a young person beyond their breaking point.
Family issues, particularly parental disputes or divorce, can also contribute to emotional distress.
Romantic rejection, particularly a first heartbreak, is one of the most common and emotionally intense triggers for young people. Adolescents often experience their first romantic relationships with immense intensity, and when these relationships end, it can feel like the end of the world. Many young people’s sense of identity and self-worth becomes closely tied to their romantic relationships, and a breakup or rejection can lead to overwhelming feelings of worthlessness, despair, and hopelessness. For some, this emotional pain can feel unbearable, especially when combined with other stressors in their lives.
Academic pressure is another recurring theme when young people talk about their stressful situations. Students often feel that their worth is tied to their performance, leading to immense stress. When combined with other stressors like friendship or family issues, the result can be overwhelming despair. We must also consider how these pressures interact with individual vulnerabilities, such as a predisposition to anxiety or depression, to fully understand why some youths are more affected than others.
Identity confusion is also a significant factor. Adolescence is a time of exploration, especially concerning personal identity, gender identity, and sexual orientation. For some, navigating these aspects of themselves can lead to significant distress, particularly if they feel unsupported or misunderstood.
Child abuse—whether physical, emotional, or sexual—can create overwhelming feelings of worthlessness and despair. Studies have shown that children who experience abuse are significantly more likely to develop mental health issues, including depression and anxiety, which are risk factors for suicide. The trauma from abuse can worsen hopelessness, making it difficult for these youths to see a future free from pain.
Family issues, particularly parental disputes or divorce, can also contribute to emotional distress. While not all divorces lead to emotional distress, the instability or conflict surrounding a family breakdown can be deeply unsettling for young people, potentially leading to suicidal thoughts.
It is important to understand that children and youths often face more than one stressor at a time, and these stressors can accumulate, making the situation feel even more overwhelming and inescapable. By recognising the complex interplay of mental health disorders, environmental factors, stressors, and individual vulnerabilities, we can better appreciate the depth of the challenges that many young people face.
Social Media’s Impact on Youth Mental Health
In a world where young people already face immense pressure, social media often amplifies their challenges. It’s not just a space for connection—it’s a constant stream of comparison, where vulnerable youths measure their lives against the carefully curated, often unattainable standards set by their peers.
Many of the young patients I’ve seen talk about how they feel ‘less than’ when scrolling through platforms like Instagram and TikTok. While these platforms can offer a sense of connection, they can also foster deep feelings of inadequacy. For youths already struggling with self-esteem or personal challenges, these comparisons can be devastating. The image of success, beauty, and happiness they see online becomes yet another unattainable goal—further driving feelings of worthlessness.
Cyberbullying is another significant issue that I have encountered in my practice. The anonymity of the internet allows bullies to harass others with little fear of consequences. Victims of cyberbullying often feel isolated and powerless, trapped in a cycle of psychological distress. The pressure to maintain a certain image online, combined with the fear of public humiliation, can push vulnerable youths toward suicidal thoughts as they see no way to escape the relentless negativity.
As a parent, it’s vital to engage in open conversations with your children about their online experiences. Rather than imposing strict bans on screen time, which may feel punitive, encourage your children to share what they see and how it makes them feel. Creating a safe space for these discussions can help them develop a healthy perspective on social media and reduce the impact of negative comparisons.
In a world where young people already face immense pressure, social media often amplifies their challenges.
Supporting Those Affected: The Role of Postvention
Postvention, the support provided to those affected by a suicide, is a crucial yet often overlooked aspect of suicide prevention. The impact of a suicide extends far beyond immediate family members, affecting friends, classmates, teachers, and even acquaintances. In my own experience, I witnessed this firsthand when my daughter lost a friend after a fall from heights. I was heartened to see that the school had structured interventions in place to support classmates and teachers during this difficult time.
However, it’s important to remember that structured postvention processes often focus on those directly involved in formal settings, such as schools. Other social groups that are equally affected by the suicide may be overlooked. These include peers from enrichment classes, playground friendships, virtual friend groups, and other less formal social circles. These groups can be just as devastated by the loss, and it is essential to extend postvention efforts to these communities as well.
Effective postvention can take many forms. Schools can start by providing immediate mental health support, such as on-site counselors, and creating spaces where students can talk openly about their grief. Peer support groups can also be invaluable in helping young people process their emotions together. Schools and communities should work to destigmatise conversations about suicide and loss, ensuring that students feel safe expressing their feelings without fear of judgment. Another critical step is offering long-term support—grief doesn’t disappear after a few weeks. Schools and community organisations should follow up with affected youths in the months after a suicide, helping them manage their ongoing emotions.
Just as important as support in schools is the involvement of families in the healing process. Parents and guardians are often a young person’s primary emotional support, and it is essential that they be part of the conversation. Family members should be prepared to discuss the loss in a way that is developmentally appropriate for their child’s age and emotional maturity. Younger children may not fully understand the permanence of death and might express their grief through behavior changes or play, while adolescents might need space to process their more complex emotions, often experiencing a heightened sense of vulnerability. Parents should create a safe, open environment where their child feels supported in sharing their feelings without fear of dismissal.
This is where age-appropriate conversations become so vital. Discussing suicide and loss with children and adolescents requires sensitivity, but it’s necessary to ensure they feel seen and understood. Younger children might need simple explanations, focusing on reassurance and security, while older youths may need a space to explore their feelings more deeply. It’s crucial for parents to acknowledge their child’s emotions, validate their pain, and provide ongoing support as grief evolves.
By providing compassionate and consistent postvention support, we can help those left behind heal from their grief and prevent further emotional distress. It’s vital to remember that postvention is not just about reacting to loss but about reinforcing the connections and resilience that can help prevent future tragedies. Families, schools, and communities must work together to provide a holistic, age-appropriate approach to support, ensuring no young person feels isolated in their grief.
Parents need to foster open communication, ensuring that their children feel safe to express their fears and anxieties.
Taking Action: Preventing Youth Suicide Together
Preventing youth suicide demands a collective effort. Families play a pivotal role in the well-being of young people. Parents need to foster open communication, ensuring that their children feel safe to express their fears and anxieties. This involves creating a home environment where emotional expression is encouraged and where children know they will be supported and not judged when they share their struggles. It’s equally important for parents to be aware of the signs of distress—such as changes in mood and behavior, withdrawal from social activities, or declining academic performance—and to be proactive in offering emotional support or seeking professional help when needed.
Schools must prioritise mental health by creating supportive environments that recognise the importance of emotional well-being alongside academic success. Schools should work to reduce the stigma of help-seeking and suicide prevention. Teachers and other staff need to be trained to identify signs of distress and intervene appropriately. Additionally, schools can incorporate programs that teach coping mechanisms and stress management skills, helping students build resilience in the face of challenges.
As a broader community, we must challenge the societal norms that contribute to the immense pressure on young people. This includes rethinking our definitions of success and ensuring that mental health resources are accessible and timely. Public awareness campaigns can play a significant role in changing perceptions about mental health and reducing stigma. Policymakers, too, have a crucial role to play in creating supportive frameworks that address the root causes of youth suicide—such as reducing academic pressure, combating child abuse, and regulating the impact of social media.
Addressing youth suicide is a daunting task, but by tackling the root causes, fostering communication, and creating supportive environments, we can help our young people find hope and resilience. Everyone has a role in this effort because, ultimately, it is the collective compassion and determination of the community that will make the difference.
Where to get help:
Mental Well-being
Institute of Mental Health’s Mental Health Helpline: 6389-2222 (24 hours)
Samaritans of Singapore: 1-767 (24 hours) / 9151-1767 (CareText via WhatsApp)
Singapore Association for Mental Health: 1800-283-7019
Silver Ribbon Singapore: 6386-1928
Tinkle Friend: 1800-274-4788
Community Health Assessment Team 6493-6500/1
Counselling
TOUCHline (Counselling): 1800-377-2252
TOUCH Care Line (For Seniors & Caregivers): 6804-6555
Obsessive Compulsive Disorder—Myths and Misconceptions
Obsessive Compulsive Disorder—Myths and Misconceptions
Obsessive-Compulsive Disorder (OCD) is a complex and often debilitating mental health condition that affects millions of people around the world.
Posted on 25 Jun 2024
Written by Dr Jared Ng, Connections MindHealth
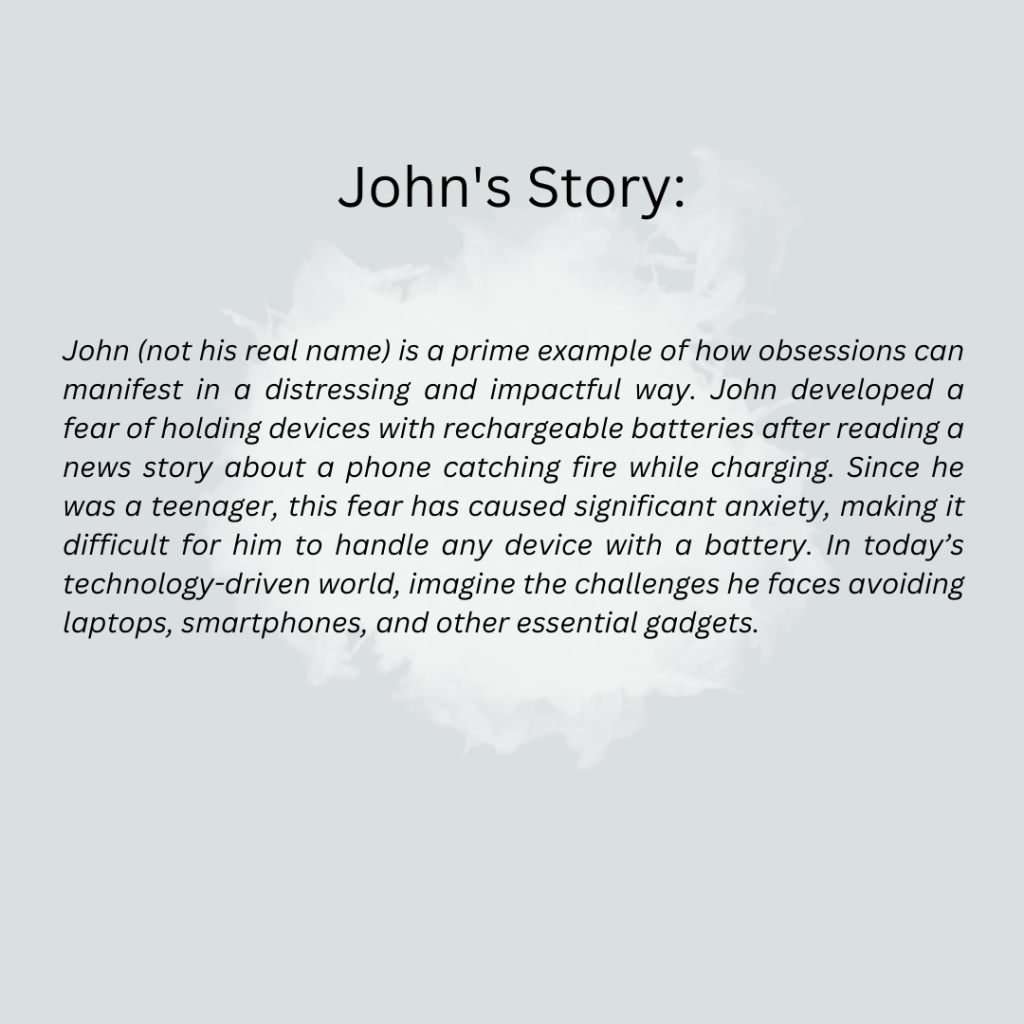
Obsessive-Compulsive Disorder (OCD) is a complex and often debilitating mental health condition that affects millions of people around the world. The 2016 Singapore Mental Health Study (SMHS) highlighted OCD as one of the top three most common mental disorders in the country [1]. The findings revealed that approximately one in every 28 adults in Singapore has been impacted by OCD, sparking discussions that Singapore might be the “OCD capital” of the world.
Characterised by persistent, unwanted thoughts (obsessions) and repetitive behaviours or mental acts (compulsions), OCD can significantly interfere with a person’s daily activities and quality of life. These obsessions and compulsions are not simply excessive worries about real-life problems or personal quirks; they are intense, consuming, and distressingly intrusive.
Despite its prevalence and severity, numerous myths and misconceptions about OCD persist, which can lead to stigma, misdiagnosis, and inadequate treatment. The 2016 SMHS suggested that the duration of untreated OCD was slightly more than 10 years, underscoring the critical need for awareness and timely intervention. Misconstruing OCD and its impacts trivialises the condition and obscures its true nature [2], preventing those affected from seeking help or receiving the empathy and support they desperately need.
This article aims to debunk some of the biggest myths about OCD and provide a clearer picture of what the disorder is. By spreading accurate information and fostering a better understanding of OCD, we hope to create a more compassionate environment that encourages those affected to seek treatment and supports them on their road to recovery.
Understanding OCD; The relationship between Obsession and Compulsion
One of the core aspects of Obsessive-Compulsive Disorder (OCD) that is often misunderstood is the distinction and relationship between obsessions and compulsions. These two components are the hallmark features of OCD, but they manifest differently and serve different psychological purposes in the disorder.
Obsessions:
Obsessions are involuntary, persistent thoughts, images, or impulses that intrude into a person’s mind and cause significant anxiety or distress. These are not simply excessive worries about real-life problems but are often irrational or exaggerated fears. People with OCD typically recognise that their obsessions are created in their minds but are unable to control or dismiss them.
Examples of less visible obsessions include:
Fear of accidentally harming oneself or others, even in “absurd” or unlikely scenarios.
Intrusive sexual thoughts or images that are distressing.
Obsessions with symmetry or exactness, where a slight imperfection can trigger intense discomfort.
Fears of shouting obscenities or acting inappropriately in public which lead to social withdrawal.
Compulsions:
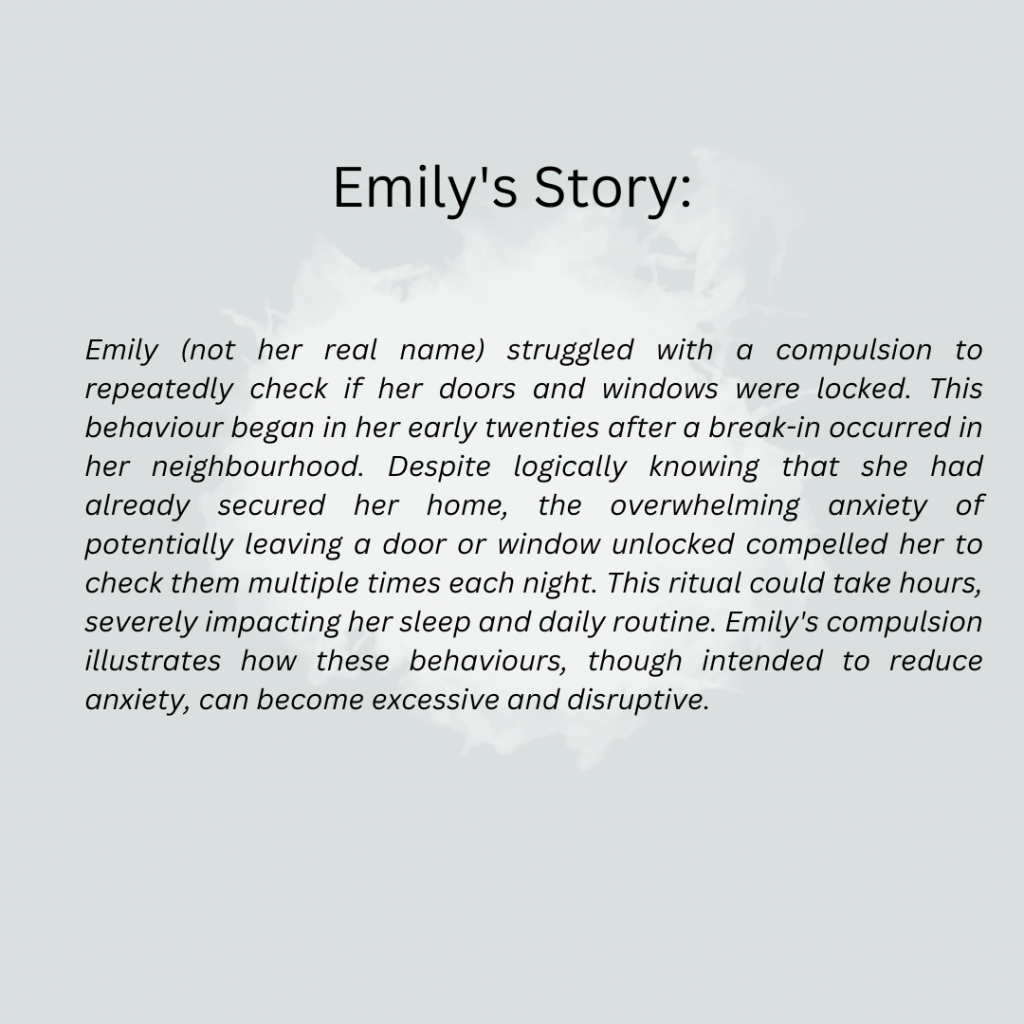
Compulsions are repetitive behaviours or mental acts that a person feels compelled to perform in response to an obsession or according to rigid rules. The primary purpose of these compulsions is to prevent or reduce the distress caused by the obsessions or to prevent a feared event or situation; however, these behaviours are either not connected logically to the feared event or are excessive.
Examples of less visible compulsions include:
Mental rituals, such as repeating certain words or phrases in one’s mind to ward off harm or bad luck.
Counting objects or performing tasks in certain numbers to “neutralise” the anxiety associated with an obsession.
Rearranging or organising items until they feel “just right” to alleviate the distress of imperfection.
Silently praying or performing rituals that cannot be observed by others, which can often go unnoticed.
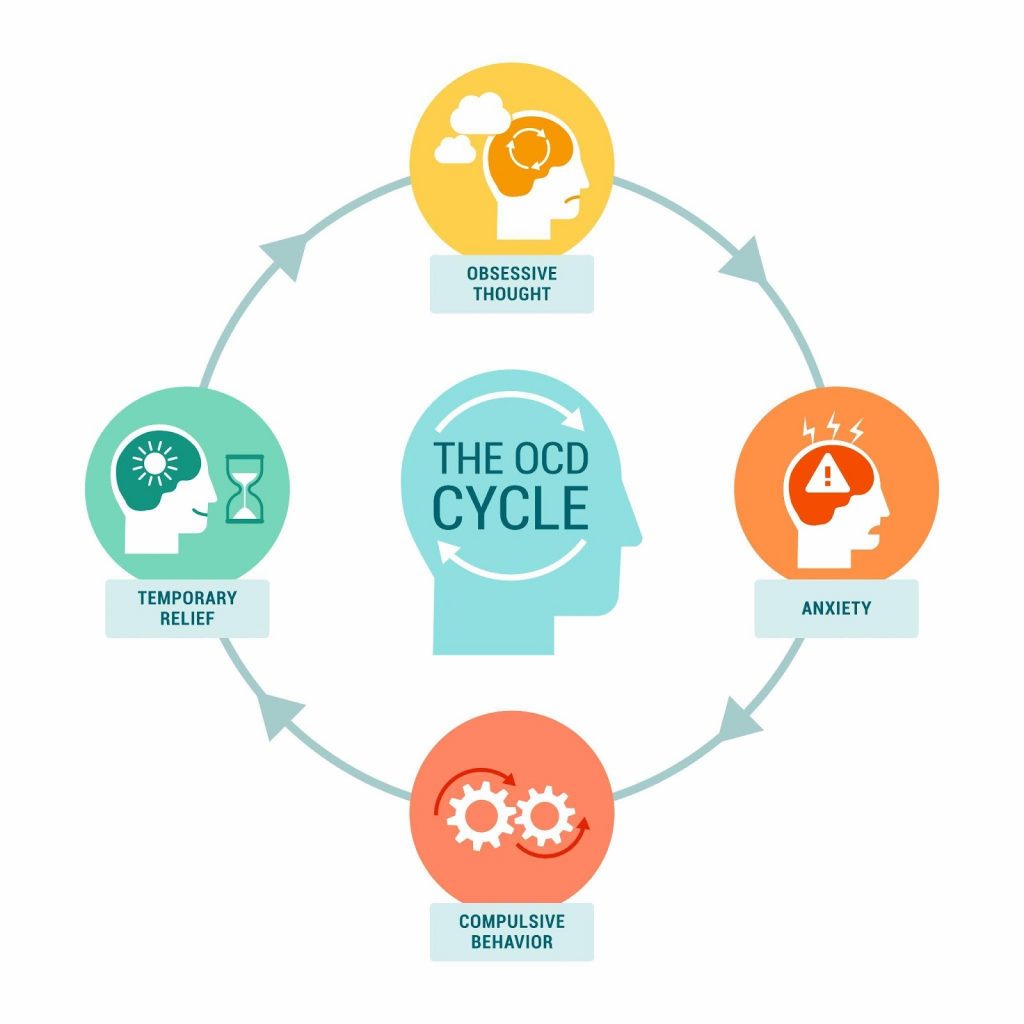
The relationship between obsessions and compulsions in OCD is one of a problematic cycle. Obsessions fuel anxiety, which compels the individual to engage in compulsive behaviours. These compulsions temporarily reduce the anxiety but reinforce the obsession, which makes it even stronger. This creates a vicious cycle that can escalate and become more debilitating over time.
OCD can be understood as a looping cycle of obsession, anxiety, compulsion and relief.
Dispelling Popular Myths: The Realities of OCD
Myth 1: OCD is just about being overly tidy and organised
One of the most common misconceptions about Obsessive-Compulsive Disorder (OCD) is that it solely manifests as a preoccupation with cleanliness and a need for order. This stereotype is often perpetuated by media portrayals and casual references that equate being meticulous or neat with having OCD. However, this simplistic view fails to capture the complexity and distress that characterise the disorder.
Popular culture’s portrayal of OCD undermines the complex and debilitating nature of OCD
Comparison with Normal Tidiness:
While many people prefer a clean and organised environment, those with OCD experience severe anxiety if things are not “just right.” For example, a person without OCD might feel satisfied after tidying up their desk, but someone with OCD might spend hours arranging and rearranging items to achieve a sense of relief from their distressing thoughts.
OCD is a clinical condition marked by severe and intrusive obsessions—unwanted thoughts, images, or urges that repeatedly enter the mind and cause significant anxiety [3]. These obsessions are coupled with compulsions, which are behaviours an individual feels compelled to perform in an attempt to reduce stress or prevent some dreaded event or situation, regardless of whether these outcomes are realistic.
The manifestations of OCD can be extraordinarily diverse. Beyond the well-known compulsions related to cleanliness, such as hand-washing or sanitising, OCD can involve:
[wpcode id=”1826″]
OCD encompasses a wide range of symptoms beyond cleanliness obsessions, including behaviours like hoarding and compulsive checking.
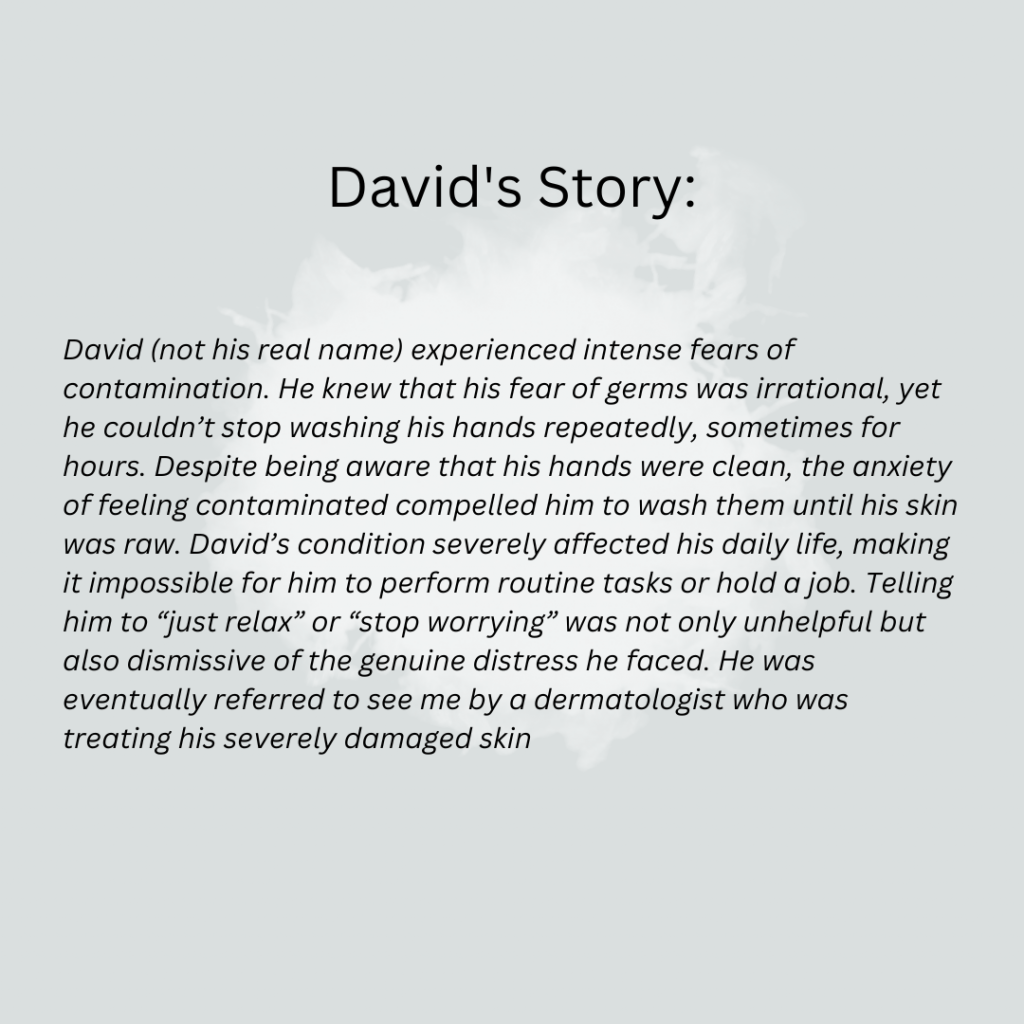
Myth 2: People with OCD just need to relax and stop worrying
A common but harmful misconception about Obsessive-Compulsive Disorder (OCD) is the notion that individuals can simply choose to ‘relax’ or stop worrying to overcome their symptoms. This belief undermines the serious nature of OCD and suggests that it is within the individual’s control to stop their obsessive thoughts and compulsive behaviours. In reality, OCD is a deeply ingrained disorder with complex biological and psychological roots, and it is not about lacking willpower or personal strength.
Biology of OCD Explained:
OCD has a significant biological basis. Research has shown that genetic factors play a crucial role in the development of the disorder, with individuals having a higher risk of developing OCD if a close family member also has the condition [8]. Neuroimaging studies have revealed that people with OCD often have differences in certain areas of the brain, including the orbitofrontal cortex, anterior cingulate cortex, and basal ganglia [9]. These brain regions are involved in decision-making, learning from mistakes, and controlling repetitive behaviours. Abnormalities in these areas can contribute to excessive doubts, compulsive checking, and the intense need to perform rituals that are characteristic of OCD.
Serotonin and Brain Function:
The role of neurotransmitters, particularly serotonin, has also been highlighted in the pathology of OCD [10]. Serotonin is crucial for mood regulation and decision-making processes. Imbalances or disruptions in serotonin levels can exacerbate the symptoms of OCD, which can result in increased anxiety and the compulsion to perform certain rituals [11]. This is why medications that target serotonin levels, such as SSRIs (selective serotonin reuptake inhibitors), are often effective in managing OCD symptoms.
Psychological Factors:
From a psychological perspective, OCD is believed to be influenced by behavioural, cognitive, and environmental factors. For example, behavioural theory suggests that compulsions are developed to reduce the anxiety caused by obsessions temporarily [12]. Cognitively, people with OCD may have maladaptive beliefs about responsibility and harm, overestimating the danger in certain situations and their role in preventing it. This can lead to excessive checking, hoarding, or other compulsive behaviours.
Why It’s Not About Willpower:
Telling someone with OCD to stop worrying or to relax is akin to telling someone with asthma to breathe normally during an asthma attack—neither helpful nor feasible. OCD is not a disorder that can be controlled or willed away by the individual. It requires professional treatment, including therapy and sometimes medication, to manage effectively.
Understanding these biological and psychological underpinnings of OCD helps highlight why reducing it to an issue of willpower is not only incorrect but also detrimental. It diminishes the real struggles experienced by those with the disorder and can prevent individuals from seeking the appropriate, evidence-based treatments that they need.
Myth 3: OCD is not a serious disorder
Contrary to the dismissive views that label Obsessive-Compulsive Disorder (OCD) as a minor annoyance or a mere personality quirk, OCD is a serious psychiatric condition recognised for its serious impact on daily functioning and overall quality of life. The idea that OCD is not a significant health issue is not only inaccurate but also diminishes the real and sometimes severe challenges faced by those who live with the disorder.
According to the World Bank and the World Health Organization, OCD is the tenth leading cause of disability globally, and for women aged 15 to 44 years, it ranks fifth. [13]. Studies have shown that individuals with OCD can experience a reduction in quality of life that is comparable to or even greater than those suffering from chronic physical conditions like diabetes [14]. The economic impact is also significant, with many individuals facing challenges in maintaining consistent employment and managing healthcare expenses related to their condition.
The data and real-life impacts illustrate that OCD is undoubtedly a serious disorder, deserving of the same attention and medical care as any other significant health issue.
Impact of OCD on Daily Life:
OCD can severely disrupt daily activities by making routine tasks extraordinarily difficult and time-consuming. For many individuals, the intense need to perform compulsive rituals—such as repeated hand washing, checking, or arranging items in a specific order—can take up several hours of their day, which severely disrupts their personal, professional, and social lives. The distressing nature of obsessive thoughts can also lead to heightened anxiety, pervasive feelings of disgust, or even a paralysing fear of harming others inadvertently. These experiences can restrict individuals’ ability to function in work settings, participate in social activities, and maintain relationships, which often leads to isolation and loneliness.
Mental Health Consequences:
The constant battle with obsessive thoughts and compulsive behaviours can lead to significant emotional distress. Many individuals with OCD experience co-occurring mental health conditions, such as depression and anxiety disorders. The relentless nature of OCD can contribute to feelings of hopelessness and helplessness, which are key risk factors for depressive symptoms and suicidal ideation. Furthermore, the stigma associated with mental health, particularly around a misunderstood condition like OCD, can exacerbate feelings of shame and inadequacy, hindering individuals from seeking help and support.
Obsessive-Compulsive Disorder (OCD) is not only a complex disorder in its own right, but it is also frequently accompanied by other psychological conditions [15]. This coexistence of multiple disorders, known as comorbidity, can complicate diagnosis and treatment, and affect the overall prognosis of those affected. Understanding the relationship between OCD and its comorbid conditions is crucial for developing comprehensive treatment plans that address all aspects of a patient’s mental health.
Common Comorbid Conditions with OCD:
Anxiety Disorders: OCD is often found alongside other anxiety disorders, such as Generalized Anxiety Disorder (GAD) [16], Panic Disorder [17], and Social Anxiety Disorder [18]. The overlap is understandable, given that both OCD and other anxiety disorders involve chronic worry and fear. However, OCD is distinct in that the anxiety typically stems from intrusive thoughts (obsessions) and is temporarily alleviated by specific actions (compulsions).
Depression: Depression is one of the most common comorbid conditions with OCD [19]. The relentless nature of OCD symptoms often leads to feelings of despair and hopelessness, which can evolve into clinical depression. The presence of depression in OCD patients can make symptoms worse and recovery more challenging, as it can sap motivation and increase feelings of worthlessness.
Eating Disorders:Eating disorders [20], particularly those involving ritualistic behaviour around food and body image, such as Anorexia Nervosa and Bulimia Nervosa, can also co-occur with OCD. The obsessive thoughts and compulsive behaviours seen in eating disorders can mirror the pattern of symptoms experienced in OCD, reflecting a shared foundation of anxiety and control issues.
Tic Disorders: Particularly in pediatric populations, there is a significant overlap between OCD and tic disorders, including Tourette Syndrome [21]. Both conditions involve repetitive behaviours, although the compulsions in OCD are typically linked to obsessional thoughts, whereas tics are often involuntary and not connected to obsessions.
Attention Deficit Hyperactivity Disorder (ADHD): Although seemingly counterintuitive due to ADHD’s association with impulsivity (opposite of OCD’s compulsivity), there is a noteworthy rate of comorbidity [22]. The shared features may include high levels of inattention, poor impulse control, and executive functioning problems.
Autism Spectrum Disorder (ASD): There is a considerable overlap between OCD and ASD. Individuals with ASD may engage in repetitive behaviours and routines similar to OCD compulsions, but the motivations behind these behaviours differ. Understanding the distinctions and overlaps is crucial for accurate diagnosis and treatment.
Autoimmune Conditions: Paediatric Autoimmune Neuropsychiatric Disorders Associated with Streptococcal Infections (PANDAS) is a condition where streptococcal infections lead to the sudden onset or worsening of OCD symptoms in children. This condition highlights the complex interplay between infections and psychiatric symptoms, necessitating a multidisciplinary approach to treatment.
Depression is a common comorbidity for individuals with OCD, which often exacerbates the challenges they face.
Treatment and Management of OCD
The presence of comorbid conditions in individuals with OCD requires a more comprehensive treatment approach. For instance, a treatment strategy that only addresses OCD may not be effective if the patient is also experiencing major depressive disorder. In such cases, a combination of medications, along with therapy tailored to address both OCD and depression, may be necessary.
Moreover, the treatment of one condition can sometimes improve the symptoms of the other. For example, the techniques used in CBT for managing anxiety can also be beneficial in controlling OCD symptoms. However, healthcare providers must monitor all conditions closely and adjust treatment plans as necessary to address the full scope of a patient’s mental health needs.
Effective treatment and management of Obsessive-Compulsive Disorder (OCD) are critical for improving the quality of life for those affected by the disorder. Modern treatment methods, professional help, and support from loved ones form the cornerstone of successful management strategies for OCD. Understanding these elements can empower individuals and their families to seek the right kind of help and support needed.
Cognitive-Behavioral Therapy (CBT): CBT is one of the most effective treatment options for OCD, particularly a specialised form known as Exposure and Response Prevention (ERP) [23]. ERP involves exposing the person to the thoughts, images, objects, and situations that make them anxious or trigger their OCD symptoms. The key is to encourage the individual not to engage in the compulsive behaviour typically performed in response to anxiety. Over time, ERP can help reduce the compulsive behaviours associated with the triggers.
Medication: Medications, especially those that increase the brain’s serotonin levels, are often prescribed in conjunction with therapy. Selective Serotonin Reuptake Inhibitors (SSRIs) are the most commonly used medications for treating OCD, helping to manage symptoms by balancing neurotransmitters [24]. In some cases, other types of psychiatric medications may be recommended depending on the individual’s symptoms and response to SSRIs. These include:
○ Tricyclic Antidepressants (TCAs): Clomipramine is a TCA that has been found to be effective in treating OCD. It works by affecting serotonin levels in the brain, similar to SSRIs, but can also influence other neurotransmitters. However, TCAs can have more pronounced side effects, such as dry mouth, constipation, and dizziness, which need to be carefully managed.
○ Antipsychotics: In some cases, antipsychotic medications such as risperidone or aripiprazole may be prescribed as adjunctive therapy, particularly if the patient does not respond adequately to SSRIs alone. These medications can help reduce intrusive thoughts and compulsive behaviours but come with potential side effects like weight gain, sedation, and metabolic changes.
○ Benzodiazepines: While not typically first-line treatments for OCD, benzodiazepines like clonazepam can be used short-term to help manage severe anxiety and agitation associated with the disorder. These medications are usually prescribed with caution due to their potential for dependence and tolerance.
○ Other Antidepressants: Some other antidepressants, such as Serotonin and Norepinephrine Reuptake Inhibitors (SNRIs), may also be effective for treating OCD symptoms in patients who do not respond to SSRIs. These medications work by affecting multiple neurotransmitters, which can be beneficial but also require careful monitoring for side effects.
Psychiatrists must balance the benefits of these medications against their possible side effects to achieve the best possible outcome for the patient. This involves careful monitoring and adjusting dosages or changing medications as needed to minimize side effects while effectively managing symptoms.
Combination Therapy: Often, a combination of CBT and medication provides the best results. This approach addresses both the behavioural and biochemical aspects of the disorder, providing a comprehensive management strategy.
Importance of Seeking Professional Help
Managing OCD typically requires more than just willpower or self-help strategies—it needs professional intervention. Mental health professionals can provide a diagnosis, recommend appropriate treatment modalities, and adjust therapies as needed based on how the patient responds over time. Professional guidance is crucial because it ensures that treatment is tailored to the individual’s specific symptoms and severity, which can significantly enhance the effectiveness of the treatment.
Seeking professional help is crucial for OCD patients, as it provides specialised therapies and support essential for managing the disorder effectively.
Encouraging Support from Family and Friends
Support from family and friends is extremely valuable in the treatment of OCD. A supportive social network can help reduce the stigma and isolation often associated with this disorder. Family members and friends can also play a proactive role by encouraging adherence to treatment regimens, providing transportation to therapy sessions, or simply being there to listen in a non-judgmental manner.
Education: It’s helpful for family and friends to educate themselves about OCD to better understand the challenges and behaviours associated with the disorder. This knowledge can foster patience and empathy, key components of support.
Participating in Therapy: Sometimes, therapists may involve family members in sessions to improve understanding and communication around the behaviours and needs associated with OCD.
Advocacy: Loved ones can also serve as advocates for individuals with OCD, helping them navigate healthcare systems and advocating for necessary accommodations at school or work.
In conclusion, the treatment and management of OCD involve a multifaceted approach that includes advanced therapeutic techniques, appropriate medication, and a strong support system. With the right combination of these elements, individuals with OCD can lead fulfilling lives despite the challenges posed by the disorder.
Moving Beyond Misconceptions
In this article, we have tackled some of the most persistent myths and misconceptions surrounding Obsessive-Compulsive Disorder (OCD). These myths not only skew public perception but also contribute to the stigma and misunderstandings that can significantly impact those living with OCD. By debunking these myths, we aim to foster a more accurate and compassionate understanding of the disorder, highlighting its complexity and the real challenges faced by those affected.
Our society stands to benefit greatly from a deeper understanding and empathy towards mental health issues, particularly OCD. Empathy begins with education and awareness, which can break down the barriers of ignorance and fear that often surround mental health disorders. We encourage everyone to advocate for and promote mental health education in their communities, which can transform public attitudes and make a real difference in the lives of those affected.
Educate Yourself and Others: Continue learning about OCD beyond this article. Education is a powerful tool for changing perceptions and promoting an environment of support and understanding.
Support Mental Health Initiatives: Includes participating in community awareness events, supporting mental health non-profits, or advocating for policies that improve mental health care, your involvement can contribute to a larger change.
Show Compassion: If you know someone struggling with OCD, offer your understanding and support. Sometimes, simply being there to listen without judgment can make a significant difference.
Seek Professional Help if Needed: If you or someone you know is battling OCD, encourage seeking help from mental health professionals. Early intervention can lead to better outcomes.
Books like The Man Who Couldn’t Stop by David Adam and Brain Lock by Jeffrey M. Schwartz
By addressing these myths and supporting those affected by OCD, we can create a more inclusive and supportive community. Let’s commit to being part of the solution, promoting understanding, and providing educated support to transform how we deal with OCD in society.
References
Subramaniam, M., Abdin, E., Vaingankar, J. A., Shafie, S., Chua, B. Y., Sambasivam, R., Zhang, Y. J., Shahwan, S., Chang, S., Chua, H. C., Verma, S., James, L., Kwok, K. W., Heng, D., & Chong, S. A. (2019). Tracking the mental health of a nation: Prevalence and correlates of mental disorders in the second Singapore mental health study. Epidemiology and Psychiatric Sciences, 29, e29. https://doi.org/10.1017/S2045796019000179
Kaur, R., Garg, R., & Raj, R. (2023). Quality of life among patients with obsessive compulsive disorder: Impact of stigma, severity of illness, insight, and beliefs. Industrial Psychiatry Journal, 32(1), 130–135. https://doi.org/10.4103/ipj.ipj_22_22
Stein, D. J., Costa, D. L. C., Lochner, C., Miguel, E. C., Reddy, Y. C. J., Shavitt, R. G., van den Heuvel, O. A., & Simpson, H. B. (2019). Obsessive–compulsive disorder. Nature Reviews. Disease Primers, 5(1), 52. https://doi.org/10.1038/s41572-019-0102-3
Strom, N. I., Soda, T., Mathews, C. A., & Davis, L. K. (2021). A dimensional perspective on the genetics of obsessive-compulsive disorder. Translational Psychiatry, 11(1), 1–11. https://doi.org/10.1038/s41398-021-01519-z
Parmar, A., & Sarkar, S. (2016). Neuroimaging studies in obsessive compulsive disorder: A narrative review. Indian Journal of Psychological Medicine, 38(5), 386–394. https://doi.org/10.4103/0253-7176.191395
Baumgarten, H. G., & Grozdanovic, Z. (1998). Role of serotonin in obsessive-compulsive disorder. The British Journal of Psychiatry. Supplement, 35, 13–20.
Żerdziński, M., Burdzik, M., Żmuda, R., Witkowska-Berek, A., Dȩbski, P., Flajszok-Macierzyńska, N., Piegza, M., John-Ziaja, H., & Gorczyca, P. (2022). Sense of happiness and other aspects of quality of life in patients with obsessive-compulsive disorder. Frontiers in Psychiatry, 13, 1077337. https://doi.org/10.3389/fpsyt.2022.1077337
Sharma, P., Rosário, M. C., Ferrão, Y. A., Albertella, L., Miguel, E. C., & Fontenelle, L. F. (2021). The impact of generalized anxiety disorder in obsessive-compulsive disorder patients. Psychiatry Research, 300, 113898. https://doi.org/10.1016/j.psychres.2021.113898
Endrass, T., Riesel, A., Kathmann, N., & Buhlmann, U. (2014). Performance monitoring in obsessive–compulsive disorder and social anxiety disorder. Journal of Abnormal Psychology, 123(4), 705–714. https://doi.org/10.1037/abn0000012
Tibi, L., van Oppen, P., van Balkom, A. J. L. M., Eikelenboom, M., Rickelt, J., Schruers, K. R. J., & Anholt, G. E. (2017). The long-term association of OCD and depression and its moderators: A four-year follow up study in a large clinical sample. European Psychiatry, 44, 76–82. https://doi.org/10.1016/j.eurpsy.2017.03.009
Beyond the Stereotype: Confronting the Mid-life Crisis and Depression among Men
Beyond the Stereotype: Confronting the Mid-life Crisis and Depression among Men
Commonly experienced in the lives of men around their middle age, goes beyond mere acts of reckless behaviours. Find out more in this article.
Key takeaways
Mid-life crises in men are often existential struggles marked by unspoken psychological turmoil, grappling with aging, mortality, and unfulfilled dreams, potentially leading to depression
Depression in middle-aged men may not present as classic symptoms but instead manifests subtly through irritability, excessive drinking, and social isolation, highlighting the need for better recognition of these signs.
Societal pressures and stereotypes discourage men from seeking help, contributing to higher suicide rates, underscoring the importance of mental health support and interventions like counseling, therapy, and self-care strategies for men facing mid-life challenges.
Posted on 4 Jun 2024
Written by Dr Jared Ng, Connections MindHealth
“Mid-life crisis” – a term casually thrown around in popular culture is often depicted as a time of impulsive decision-making, like buying a flashy sports car, ending years of marriage to engage with younger women, or taking up an extreme hobby. For many men, the deeper psychological struggle is seldom acknowledged. It’s these unspoken realities we need to confront.
This so-called “crisis”, commonly experienced in the lives of men around their middle age, goes beyond mere acts of reckless behaviours. It is an existential struggle, a silent cry for help as they grapple with aging, their own mortality, a sense of lost youth, and unfulfilled dreams. In many cases, this mid-life crisis may act as a trigger or precursor to depression, a debilitating condition that remains under-discussed and poorly understood when it comes to men.
Mid-life crises in men involve deep psychological struggles and can lead to depression.
Depression in many of us men does not necessarily present itself in textbook terms; it’s not always the profound sadness or hopelessness that we read in books or off medical websites. Instead, the condition may manifest subtly – an increasingly quick temper, heightened irritability, excessive drinking, a sense of losing control, dwindling work performance, and social isolation. The ability to spot these symptoms is the first step in recognizing the suffering that many middle-aged men are enduring.
Stereotypes and societal pressures seem to play a significant role in this complex problem. Men are often conditioned by society to be the ‘strong’ ones, taught to mask their struggles and suppress their feelings. As a result, they are less likely to seek help due to fear of appearing weak or vulnerable. A heartbreaking consequence of these challenges is the higher proportion of suicides happening in men compared to women – a troubling statistic in many parts of the world, including Singapore. This underscores the urgency of addressing mental health issues among men, especially those in mid-life facing a unique set of stressors.
Depression in middle-aged men often shows as irritability, drinking, and isolation.
When I think back to my patients, their stories of struggle share common threads. Marital discord, often resulting from fading passion, ill-placed romances, fraught divorces, the enormous responsibility of parenting, professional stagnation, financial problems and other life disappointments, all form part of a melancholic tapestry. As they navigate the terrain of middle age, the harsh reality of mortality, financial pressures, medication side effects, physical health changes, lifestyle factors, and hormonal changes further compound their psychological burden.
In Singapore, it’s particularly poignant to see these men, hailed as pillars of their families and societies, crumble under such weight. Yet, it’s this very reality that can propel us to institute change, to introduce a comprehensive roadmap to recovery.
As a mental health professional, I have found that a combination of medication, therapy, and self-care strategies can significantly alleviate depressive symptoms. Access to good quality counselling, psychotherapeutic treatment, and the appropriate use of medication, are extremely useful in tackling the symptoms of depression.
Societal pressures deter men from seeking help, highlighting the need for mental health support.
But equally important is the adoption of self-help strategies. I encourage my patients to establish achievable goals, create a strong support network, practice stress-management techniques, and delay significant decisions until their depressive symptoms subside. Prioritizing self-care, they learn, is as crucial as meeting work deadlines or family obligations.
The road to recovery is not linear, and relapses are part of the process. However, with timely intervention and sustained treatment, I have seen my patients reclaim their lost zeal, rekindling their passion for work, hobbies, and their relationships.
Depression does not discriminate. It can target anyone, regardless of age, gender, or status. However, by acknowledging its unique manifestations in middle-aged men, by understanding and addressing the multitude of factors contributing to its onset, we can begin to make a difference. For every man in Singapore navigating the turbulent waters of mid-life depression, remember this – it’s okay not to be okay, and help is available. You are not alone.
Empowering New Mothers: Navigating Postpartum Mental Health in Singapore
Empowering New Mothers: Navigating Postpartum Mental Health in Singapore
Through this blog, we aim to create a supportive dialogue that breaks down the barriers of silence and stigma surrounding postpartum mental health.
Posted on 8 May 2024
Written by Dr Jared Ng, Connections MindHealth
Welcoming a new life into the world is often portrayed as a time of joy and fulfilment. However, for many women, the postpartum period can bring unexpected mental health challenges. Postpartum depression, anxiety, and other mood disorders can significantly impact new mothers. Despite its prevalence, postpartum mental health remains under-discussed, particularly in places like Singapore, where traditional norms can make it challenging to address these issues openly.
Addressing mental health issues in new mothers is crucial—not just for individuals but also for public health. The implications of postpartum mental disorders extend beyond the individual, affecting infants’ development and family well-being. In Singapore, where family unity is a cornerstone of society, ensuring the mental health of new mothers is essential for nurturing healthy communities.
Through this blog, we aim to create a supportive dialogue that breaks down the barriers of silence and stigma surrounding postpartum mental health. By spreading awareness and fostering understanding, we hope to empower mothers to seek help without fear of judgment. We also aim to encourage a cultural shift — one that recognises the strength of seeking help and the importance of mental wellness for all mothers.
Postpartum depression can cause severe emotional distress and hinder a new mother’s ability to care for themselves and their newborn.
Baby Blues — Typical Mood Changes After Delivery
The arrival of a newborn brings immense joy but can also be accompanied by a range of emotions. It’s important for new mothers to understand that experiencing mood changes shortly after delivery is common. This phenomenon, known as the “baby blues“, affects up to 80% of mothers and usually occurs within the first few days to weeks after childbirth.
What are the Baby Blues?
The “baby blues” describe a short-term period of emotional instability that can include:
Mood swings: It’s normal for new mothers to experience rapid shifts in mood, going from happiness to sadness without warning.
Crying spells: Mothers may find themselves crying for no apparent reason, often triggered by something minor.
Anxiety: Many new mothers feel anxious about their baby’s well-being or their abilities as a mother.
Irritability: It’s not unusual to feel irritable or overwhelmed by the demands of caring for a newborn.
Insomnia: Some new mothers may struggle to fall or stay asleep despite feeling exhausted.
These symptoms typically peak around the fourth or fifth day after birth and subside within two weeks. The “baby blues” are believed to be caused by the dramatic hormonal changes that occur after childbirth, along with the stress and exhaustion of caring for a newborn.
Normalising the Baby Blues
Understanding that the “baby blues” are a common part of postpartum adjustment can help new mothers feel less alone and more prepared for the emotional ups and downs of early motherhood. It’s important to remember that these feelings are usually temporary and do not indicate a lack of maternal love or ability.
Beyond Baby Blues – When it is a Mental Health Disorder
While “baby blues” are common and generally short-lived, some new mothers experience more intense and persistent symptoms that indicate a more serious mental health condition. It’s crucial to differentiate between the normal emotional fluctuations of early motherhood and postpartum mental health disorders that require professional intervention. Recognising the signs of conditions like postpartum depression, postpartum anxiety, or psychosis is the first step toward seeking the necessary support and treatment for recovery. In this section, we explore these conditions in greater detail, helping new mothers and their loved ones understand when to seek help.
Postpartum depression (PPD) is the most prevalent of these conditions, characterised by persistent feelings of sadness, worthlessness, and exhaustion that go beyond the typical “baby blues.” These feelings can last weeks to months and interfere significantly with a mother’s ability to care for her child and herself.
Postpartum anxiety involves an intense, debilitating worry that is out of proportion to the actual situation. Mothers may experience severe anxiety, panic attacks, and fears about their baby’s health and well-being or their abilities as a mother [1].
Other conditions: Postpartum Psychosis is rarer but more severe, involving hallucinations, delusions, and extreme confusion. Postpartum Obsessive-Compulsive Disorder (OCD) is marked by intrusive, repetitive thoughts and fears, often centred on the baby’s safety, which the mother knows are irrational but feels powerless to stop.
Recognising the Signs
Recognising the signs of postpartum mental health issues is crucial for early intervention and effective treatment. The symptoms can be diverse, spanning emotional, physical, and behavioural changes that disrupt a new mother’s daily functioning and well-being. Here’s a detailed look at what to watch for:
Emotional Symptoms of Postpartum Depression
Persistent sadness or low mood: feelings of sadness that last most of the day, nearly every day, not just occasional blues.
Crying spells: new mothers suffering from postpartum mental health issues may experience frequent, unexplained crying that feels uncontrollable [2].
Irritability or anger: irritability or anger that is unusual or out of proportion to the situation.
Feelings of worthlessness or guilt: persistent thoughts of not being a good mother or unwarranted guilt over minor issues.
Anhedonia:anhedonia is the loss of interest or pleasure in activities previously enjoyed, including withdrawal from social interactions.
Physical Symptoms of Postpartum Depression
Fatigue: severe tiredness that doesn’t improve with rest, affecting the ability to care for oneself and the baby.
Sleep disturbances:difficulty falling asleep, staying asleep, or sleeping much more than usual, unrelated to the baby’s sleep schedule [3].
Changes in appetite: significant increase or decrease in appetite, leading to weight loss or gain unrelated to pregnancy [4].
Aches and pains: physical symptoms like headaches, stomachaches, or muscle pain without a clear physical cause.
Behavioural Symptoms of Postpartum Depression
Cognitive impairments: trouble concentrating, remembering details, or making decisions that affect daily tasks.
Anxiety and panic: excessive worry about the baby or one’s abilities as a mother, possibly escalating to panic attacks.
Obsessive thoughts: intrusive, repetitive thoughts, often about harm coming to the baby, which the mother recognises as irrational but feels powerless to control [5].
Avoidance behaviours: avoiding situations or activities due to anxiety or fear, including avoiding caring for the baby.
As mentioned, some of these symptoms can be a normal part of adjusting to motherhood for many. However, when they are intense, persistent, and interfere with daily life, they may indicate a more serious postpartum mental health issue. Early detection and intervention are crucial to managing these symptoms effectively.
The “baby blues” are a brief period of sadness and mood swings after childbirth, while postpartum depression involves persistent emotional distress that can impair functioning.
From Hormones to Social Pressures—What Contributes to Postpartum Mental Health Challenges?
To effectively address and mitigate postpartum mental health challenges, it is essential to understand the varied risk factors that can influence a new mother’s well-being. These risks are multifaceted and include biological, psychological, and social dimensions, each contributing to postpartum mental health concerns.
In Singapore, additional cultural factors also play a critical role in shaping the experiences and expectations placed on new mothers. By examining these elements, we can better support and empower mothers and ensure they receive the care needed during this transformative period.
Biological factors
Hormonal changes: The rapid fluctuation in hormones such as oestrogen and progesterone after childbirth can significantly impact mood and is a major biological trigger for postpartum depression and anxiety [6].
Genetics: A family history of depression or other mental health disorders can increase a woman’s risk of experiencing similar issues postpartum [7].
Physical recovery from childbirth: Complications during delivery, such as prolonged labour or a caesarean section, and physical recovery issues, such as chronic pain or fatigue, can contribute to the development of postpartum mental health issues [8].
Prolonged labour or physical recovery challenges post-delivery can heighten the risk of developing postpartum mental health issues by increasing stress and physical discomfort.
Psychological factors
Previous mental health issues: Women who have previously experienced mental health issues, including depression or anxiety, are at a higher risk of postpartum mental health problems.
Psychological adjustment: Difficulty adjusting to the role of motherhood, feelings of loss of identity, or lack of fulfilment in their new role can also pose significant psychological challenges.
Social factors
Support systems: A lack of adequate support from partners, family, or friends can increase the risk. This includes practical support in caring for the newborn and emotional support in dealing with the stresses of new parenthood.
Socioeconomic stressors: Financial difficulties, job security concerns, or inadequate living conditions are significant stressors that can exacerbate postpartum mental health issues [9].
Cultural Factors Specific to Singapore
High expectations and perfectionism: In Singapore’s performance-oriented society, mothers are often expected to adapt and excel quickly in their new roles. This cultural norm can lead to feelings of inadequacy and failure.
Stigma and secrecy: Mental health issues are often stigmatised, with a prevalent culture of secrecy around such topics. This can prevent new mothers from seeking the help they need, which can worsen their mental health condition.
Role of extended family: In Singapore, extended family often plays a significant role in postpartum care. While this can be a source of support, it can also lead to increased pressure and criticism, particularly from older generations with traditional views on child-rearing.
Work-life balance challenges: The pressure to return to work soon after childbirth due to economic necessity or career expectations can significantly strain mental health, especially without flexible work policies or sufficient maternity leave.
Each of these factors contributes to the postpartum mental health challenges faced by new mothers. Recognising these risks not only aids in empathy and understanding but also highlights critical areas for support and intervention, which can ensure that mothers receive the care they need during this vulnerable time.
Michelle’s Story: A Real-Life Example of Postpartum Depression in Singapore
“Michelle (not her real name), a mother of two, experienced a challenging postpartum period after delivering her daughter two weeks ago. Initially, she dismissed her sadness and irritability as normal “baby blues.” However, as the days passed, Michelle found herself overwhelmed with persistent sadness and inexplicable crying spells. She felt disconnected from her newborn and struggled with feelings of worthlessness. Her husband noticed her withdrawal from family activities and her lack of interest in things she previously enjoyed, including reading and playing with her eldest son.
Recognising that Michelle needed help, her husband encouraged her to speak with a mental health professional. Through counselling and with the support of her family, Michelle began to understand her feelings and work towards recovery. Her story is a powerful reminder that postpartum depression is a common and treatable condition and that seeking help is a sign of strength, not weakness.”
Increased pressure and criticism play a significant role in cultural factors which contribute to post-partum depression.
The Role of Fathers—Supporting New Mothers Through Postpartum Mental Health Challenges
As a father of three children, I understand firsthand the crucial role fathers can play in supporting new mothers during the postpartum period. Fathers should not be neglected when discussing postpartum mental health, as they have significant roles to play in ensuring the well-being of their partners and their children. At the same time, fathers’ mental health during this period is important too. While we will address this in more detail in a future blog post, here’s a quick teaser on how fathers can provide valuable support:
Emotional support: Fathers can offer a listening ear and be emotionally available for their partners. Simply being there to listen and offer empathy can be incredibly comforting for new mothers.
Practical assistance: Helping with household chores, diaper changes, or feeding the baby can relieve some of the burden on new mothers and allow them to rest and recover.
Encouragement to seek help: Fathers can encourage their partners to seek professional help if they notice symptoms of postpartum depression or other mental health issues. Early intervention is key to recovery, and fathers can play a pivotal role in ensuring mothers receive the care they need.
Promoting self-care: Encouraging mothers to take time for self-care, whether taking a nap or enjoying a warm bath, can significantly improve their well-being. Fathers can facilitate this by taking on additional responsibilities when needed.
Participating in parenting: Engaging in parenting activities like feeding, bathing, or soothing the baby not only strengthens the father-child bond but also provides mothers with a much-needed break.
By being supportive, understanding, and proactive, fathers can make a positive impact on their partners’ postpartum mental health and create a nurturing environment for the whole family.
Restoring Balance—Essential Strategies for Overcoming Postpartum Mental Health Challenges
Adopting a healthy lifestyle and creating a supportive network are foundational steps in the recovery journey for new mothers facing postpartum mental health challenges, including the “baby blues” and postpartum depression.
Lifestyle Adjustments and Self-Care Tips for Postpartum Depression
Rest: Sleep is crucial for emotional well-being. Encourage mothers to rest whenever possible, even if it’s just a short nap while the baby sleeps.
Support: Emotional support from family and friends can make a big difference. Simply having someone to talk to or help with household tasks can relieve stress.
Nutrition: Focus on a balanced diet rich in nutrients that support brain health and energy levels, such as omega-3 fatty acids, lean proteins, and whole grains. Encourage mothers to eat regular, nutritious meals, even if they don’t have much appetite [10].
Exercise: Regular physical activity, which has been proven to reduce symptoms of depression and anxiety [11]. Even light exercises like walking or stretching can make a significant difference.
Sleep: Prioritise sleep, when possible, as lack of sleep significantly impacts mental health and cognitive function.
Mindfulness and relaxation: Techniques like yoga, meditation, and deep-breathing exercises can reduce stress and improve overall emotional health.
Time for self-care: Taking time for self-care, even for a few minutes, can help mothers feel more balanced. This could be as simple as a warm bath or quiet time with a book.
Routine: Create a daily routine to provide structure, which can be comforting amidst the chaos of new parenthood.
Community resources: Leverage community resources such as mothers’ groups, parenting workshops, and family wellness programs. These can provide emotional support and a sense of belonging, reducing feelings of isolation.
Online support: Consider online forums and social media groups focusing on postpartum health. These platforms can offer support at any hour, particularly useful for new mothers managing unpredictable schedules.
Medical and Therapeutic Interventions for Postpartum Depression
In addition to lifestyle adjustments, medical and therapeutic interventions are sometimes required for mothers facing more serious postpartum mental health challenges.
Counselling: Professional counselling services can be invaluable, providing a safe space to discuss feelings and concerns. Cognitive Behavioral Therapy (CBT) is particularly effective for managing depression and anxiety [12].
Medication: Antidepressants may be prescribed when symptoms are moderate to severe, and they can be an essential part of treatment. It’s crucial to discuss the benefits and risks with your psychiatrist, especially when breastfeeding.
Integrated care: Integrated care programmes combine psychological therapy with support for the practical aspects of new motherhood and infant care.
Professional guidance: Mental health professionals can tailor treatment plans to individual needs and ensure mothers receive the most effective care.
Integrating these management strategies with therapeutic interventions offers a comprehensive approach to addressing postpartum mental health challenges. New mothers can actively facilitate their recovery by engaging with available resources and adopting recommended practices.
Counseling or guidance from a mental health professional can help new mothers manage postpartum depression by providing emotional support and coping strategies.
Empowering New Beginnings — Taking Action on Postpartum Mental Health
Recognising and addressing postpartum mental health issues is crucial for the well-being of new mothers and their families. The journey through motherhood can be marked by a range of emotional and psychological challenges, but no mother should have to navigate this path alone.
It is vital that mothers feel empowered to seek help and are reassured that their experiences, while unique, are shared by many others. The strength and resilience shown by mothers every day are inspiring, but even the strongest among us can benefit from support. By shedding light on these issues and offering support, we can make a difference in the lives of new mothers and help them not only endure but thrive.
References
Garapati, J., Jajoo, S., Aradhya, D., Reddy, L. S., Dahiphale, S. M., & Patel, D. J. (n.d.). Postpartum mood disorders: Insights into diagnosis, prevention, and treatment. Cureus, 15(7), e42107. https://doi.org/10.7759/cureus.42107
Baattaiah, B. A., Alharbi, M. D., Babteen, N. M., Al-Maqbool, H. M., Babgi, F. A., & Albatati, A. A. (2023). The relationship between fatigue, sleep quality, resilience, and the risk of postpartum depression: An emphasis on maternal mental health. BMC Psychology, 11(1), 10. https://doi.org/10.1186/s40359-023-01043-3
Tayhan, F., Doğan, G., Yabancı Ayhan, N., & Sancar, C. (2024). Assessment of eating disorders and depression in postpartum women. European Journal of Clinical Nutrition, 78(4), 314–319. https://doi.org/10.1038/s41430-023-01384-7
Collardeau, F., Corbyn, B., Abramowitz, J., Janssen, P. A., Woody, S., & Fairbrother, N. (2019). Maternal unwanted and intrusive thoughts of infant-related harm, obsessive-compulsive disorder and depression in the perinatal period: Study protocol. BMC Psychiatry, 19(1), 94. https://doi.org/10.1186/s12888-019-2067-x
Saraswat, N., Wal, P., Pal, R. S., Wal, A., Pal, Y., & Roohi, T. F. (2021). A detailed biological approach on hormonal imbalance causing depression in critical periods (Postpartum, postmenopausal and perimenopausal depression) in adult women. The Open Biology Journal, 9(1). https://doi.org/10.2174/1874196702109010017
Hutchens, B. F., & Kearney, J. (2020). Risk factors for postpartum depression: An umbrella review. Journal of Midwifery & Women’s Health, 65(1), 96–108. https://doi.org/10.1111/jmwh.13067
Smithson, S., Mirocha, J., Horgan, R., Graebe, R., Massaro, R., & Accortt, E. (2022). Unplanned Cesarean delivery is associated with risk for postpartum depressive symptoms in the immediate postpartum period. The Journal of Maternal-Fetal & Neonatal Medicine, 35(20), 3860–3866. https://doi.org/10.1080/14767058.2020.1841163
Karl, M., Schaber, R., Kress, V., Kopp, M., Martini, J., Weidner, K., & Garthus-Niegel, S. (2020). Precarious working conditions and psychosocial work stress act as a risk factor for symptoms of postpartum depression during maternity leave: Results from a longitudinal cohort study. BMC Public Health, 20(1), 1505. https://doi.org/10.1186/s12889-020-09573-w
Rupanagunta, G. P., Nandave, M., Rawat, D., Upadhyay, J., Rashid, S., & Ansari, M. N. (2023). Postpartum depression: Aetiology, pathogenesis and the role of nutrients and dietary supplements in prevention and management. Saudi Pharmaceutical Journal : SPJ, 31(7), 1274–1293. https://doi.org/10.1016/j.jsps.2023.05.008
Singh, B., Olds, T., Curtis, R., Dumuid, D., Virgara, R., Watson, A., Szeto, K., O’Connor, E., Ferguson, T., Eglitis, E., Miatke, A., Simpson, C. E., & Maher, C. (2023). Effectiveness of physical activity interventions for improving depression, anxiety and distress: An overview of systematic reviews. British Journal of Sports Medicine, 57(18), 1203–1209. https://doi.org/10.1136/bjsports-2022-106195
Anxiety is not just a medical term; it's a shared human experience, weaving through the lives of countless individuals in myriad, often invisible ways. In this short write-up, Dr Jared Ng sheds light on the realities of anxiety, debunking myths and exploring treatments, all while emphasizing the human experience at the heart of it all.
Key takeaways
Anxiety is a complex emotion that, when persistent and overwhelming, may indicate an anxiety disorder.
Not all anxiety is visible, and assuming so can lead to inadequate support for those silently struggling with internal distress.
Anxiety disorders represent a spectrum, each with distinct themes and symptoms, ranging from Generalized Anxiety Disorder (GAD) to Post-Traumatic Stress Disorder (PTSD).
Posted on 3 Apr 2024
Written by Dr Jared Ng, Connections MindHealth
Anxiety is not just a medical term; it’s a shared human experience, weaving through the lives of countless individuals in myriad, often invisible ways.
I am seeing a patient, Miss Sally (not her real name), a bright university graduate whose life took an unexpected turn. She was on her way to a job interview when she was unfortunately trapped in a lift for almost an hour. Sally experienced her first panic attack, marked by shortness of breath, chest discomfort, giddiness, headache, and an overwhelming fear of impending doom. She was late for her job interview and she was too discouraged to attend another session, even though the company was sympathetic.
After her traumatic experience in the life, Sally’s anxiety escalated significantly. She began to fear having more panic attacks, a concern that soon extended to various aspects of her daily life. Initially, she started avoiding taking the lift alone, a direct response to her initial panic attack. However, her anxiety gradually grew to include other enclosed spaces like public transport. This progression of her anxiety led to her avoiding leaving her house altogether, significantly restricting her day-to-day activities and impacting her overall quality of life. Her world became increasingly limited, dominated by the fear of experiencing another panic attack and the physical and emotional distress that accompanies it. Sally’s parents did not understand why their daughter could not find the job or even leave the house after graduation, and this led to conflicts between them.
Sally’s story is a stark reminder of how anxiety can envelop one’s life, casting a shadow over everyday activities and relationships. As a psychiatrist, I’ve seen how such experiences can lead to a withdrawal from social interactions, a loss of self-confidence, and a sense of isolation, even when surrounded by supportive family and friends. Some of them develop a co-morbid depressive disorder. It’s a poignant example of the hidden struggles many faces, often masked by a veneer of normalcy.
But Sally’s narrative is just one among many. Anxiety wears numerous faces – from the constant worry of generalised anxiety disorder to the specific, intense fears of phobias, or the daunting challenge of social anxiety. Each individual’s experience with anxiety is as unique as their fingerprint, yet there’s a common thread of needing understanding, support, and effective coping mechanisms.
In this short write-up, I hope to shed some light on the realities of anxiety, debunk myths, and explore the myriad of treatments available, all while keeping sight of the most important aspect – the human experience at the heart of it all.
Recognising Anxiety
Anxiety, a common yet complex emotion, is something we’ve all experienced at various points in our lives. It’s a natural response to stress, uncertainty, or fear. However, when these feelings become persistent and overwhelming, they may indicate an anxiety disorder.
Cognitively, anxiety manifests in several ways. It often appears as constant, excessive worrying about everyday activities, where the level of concern is disproportionate to the actual risk or impact. This worrying can be so intense that it interferes with the ability to focus, leading to difficulty in concentrating or a sense of the mind going blank. There’s also a tendency to anticipate the worst, even in relatively benign situations, and to struggle with decision-making due to the fear of making the wrong choice. Intrusive thoughts, which are repetitive and unwelcome, can dominate the mind, contributing to a state of constant fear or apprehension.
Behaviourally, anxiety influences our actions and choices. It often leads to the avoidance of situations or activities that trigger fear or discomfort. This avoidance can significantly restrict one’s life, limiting opportunities and experiences. Compulsive behaviors may emerge as a coping mechanism, where repetitive actions are performed in an attempt to reduce or control the anxiety. Restlessness is common, manifesting as an inability to relax or sit still, and there can be a tendency to procrastinate or have difficulty completing tasks, rooted in the anxiety itself. People with anxiety often seek reassurance from others, needing constant validation to alleviate their fears.
Physically, anxiety has a range of manifestations. It can cause palpitations or an unusually rapid heart rate, often accompanied by chest pain. Excessive sweating, unrelated to physical exertion or environmental temperature, is another common symptom. Physical signs of nervousness, such as trembling or shaking, are observable, and gastrointestinal problems like nausea, diarrhoea, or an upset stomach frequently occur. Additionally, muscle tension, leading to headaches and other physical discomforts, is often a physical representation of anxiety.
It’s important to note that these symptoms can vary widely among individuals. Not everyone with anxiety will experience all these symptoms, and their intensity and frequency can differ. Recognising these symptoms in oneself or others is vital for early identification and intervention. Understanding these signs is the first step in managing anxiety effectively, allowing for strategies and treatments to be tailored to the individual’s specific experiences and needs.
Myths, Misunderstandings and Misrepresentations About Anxiety
The term ‘anxiety‘ is commonly used to describe both everyday feelings of worry and also a clinical psychiatric condition. This dual usage can lead to misunderstandings and oversimplifications of the disorder. For instance, when anxiety is portrayed as just an extreme state of nervousness, it minimises the complex nature of anxiety disorders, which are profound mental health issues impacting one’s life, relationships, and ability to function normally.
The misconception that anxiety can be overcome solely by willpower is another simplification. It overlooks the intricate interplay of biological, psychological, and environmental factors that contribute to anxiety disorders. Effective management often requires a multifaceted approach, including psychological therapy, medication, and lifestyle adjustments. This myth also perpetuates a stigma, suggesting that those who struggle with anxiety are simply not trying hard enough, or are too “weak” mentally.
Furthermore, the belief that anxiety is always visible fails to recognise that many individuals with anxiety present a calm exterior despite experiencing intense internal distress. This can lead to underestimation of their struggle and inadequate support from others.
Given that ‘anxiety’ is used to describe both normal and pathological states, there’s a tendency to either underestimate the severity of the condition or misinterpret normal stress responses as pathological. And because everyone has experienced anxiety at some point, there may be preconceived notions about how one can ‘recover’ from it. However, the experience of anxiety is deeply personal and varies greatly from one individual to another. What may be a minor stressor for one person could be a significant source of anxiety for another. This variation in experiences can lead to misunderstandings about the nature of anxiety disorders and the challenges faced by those who struggle with them. Recognising that each person’s anxiety is unique is crucial in providing appropriate support and avoiding oversimplification of their experiences.
Types of Anxiety Disorders
Anxiety disorders are also not a monolithic condition; they represent a spectrum, each type characterised by an underlying theme of excessive fear and worry, yet presenting distinct symptoms.
Examples:
Generalised Anxiety Disorder (GAD) is characterised by chronic and pervasive worry about a range of topics, often disproportionate to the actual threat.
Panic Disorder involves recurrent, intense panic attacks with physical symptoms like shortness of breath and chest pain.
Social Anxiety Disorder is marked by a deep fear of social interactions due to concerns about judgment or embarrassment.
Specific Phobias involve irrational fears of particular objects or situations, leading to avoidance behaviors.
Obsessive-Compulsive Disorder (OCD) consists of unwanted thoughts and repetitive behaviors aimed at reducing anxiety.
Post-Traumatic Stress Disorder (PTSD) stems from traumatic experiences and includes symptoms like flashbacks and avoidance behaviors.
Sometimes symptoms don’t fit neatly into these categories, particularly when they are evolving or atypical. The focus in psychiatry is always on the individual person and their unique experiences, emphasising the dynamic and evolving nature of mental health disorders. We treat the person, not the label.
Is Anxiety Curable?
While anxiety disorders are complex and long-term conditions, there is a beacon of hope in treatment. People with anxiety disorders often respond positively to a combination of therapies. This includes pharmacological treatments i.e. medication, and non-pharmacological approaches, such as cognitive behavioral therapy and lifestyle changes. An integral part of managing anxiety is the support from one’s network – family, friends, school, colleagues, and employers. Their understanding and encouragement can significantly bolster treatment effectiveness, creating an environment conducive to recovery and well-being.
Treatment for Anxiety Disorders can be broadly divided into two categories:
Pharmacological Treatments: Medications play a significant role in managing anxiety disorders. These include Selective Serotonin Reuptake Inhibitors (SSRIs) and Serotonin-Norepinephrine Reuptake Inhibitors (SNRIs) that help balance brain chemistry. Benzodiazepines are effective for short-term relief of acute anxiety symptoms but are generally not recommended for long-term use due to the risk of dependence. Beta-blockers like Propranolol can also be prescribed to manage physical symptoms of anxiety, such as palpitations and tremors.
Non-Pharmacological Treatments: Cognitive Behavioral Therapy (CBT) is highly effective, particularly for panic disorders and generalised anxiety disorder, focusing on changing thought patterns and behaviors. Techniques like mindfulness, relaxation exercises, and exposure therapy are also integral parts of non-pharmacological treatment. Alternative therapies like hypnotherapy or brain stimulation techniques (like transcranial magnetic stimulation) have shown promise in some cases, and are being researched extensively.
Integrated Care Approach: Often, a combination of pharmacological and non-pharmacological treatments is most effective. Integrated care, which involves coordinating psychological therapy with medication management and lifestyle changes, is considered the best approach for treating anxiety disorders. This holistic approach addresses the multifaceted nature of anxiety, ensuring that treatment is tailored to the individual’s specific needs and circumstances.
Treatments can lead to significant improvements in symptoms and quality of life. However, it’s important to note that discontinuing treatment can result in a recurrence of symptoms, highlighting the need for ongoing management.
Conclusion
In closing, understanding and managing anxiety is a journey both challenging and hopeful. While anxiety disorders are complex and vary from person to person, effective treatments and supportive networks provide a pathway to better managing this condition. Through a combination of therapy, medication, and lifestyle changes, individuals can find relief and improve their quality of life. Remember, anxiety is a part of the human experience, and with the right support and interventions, it can be navigated successfully. There’s always hope and a way forward.
Epilogue
Sally’s journey towards recovery has seen significant progress thanks to a combination of medication and psychological treatment. Psychoeducation for her family played a crucial role in improving their understanding and support, which has been immensely beneficial. I’m delighted to share that Sally is now preparing to start a new job in two weeks, marking a hopeful turn in her journey.